Advanced Imaging Chips Empower Endoscopy Applications
November 08, 2019
Blog

OmniVision Technologies 0.575mm x 0.575mm OV6948 image sensor is used in its wafer-level camera module 0.65mm x 0.65mm x 1.158mm OVM6948 CameraCubeChip.
The myriad of wired systems can often be overlooked when wireless application spaces, empowered by advanced miniaturization, is at the forefront of medical technologies. In the area of medical devices, there are benefits of wired solutions, especially in fields like medical robotics, diagnostic and treatment gear, and tools for endoscopic surgery. These solutions may make for safer procedure.
Creating high-resolution medical and optical imaging solutions for endoscopic work is fraught with many issues including size, thermal management, color accuracy, among other things.
Tehzeeb Gunja, marketing manager of OmniVision Technologies, whose 0.575mm x 0.575mm OV6948 image sensor is used in its wafer-level camera module 0.65mm x 0.65mm x 1.158mm OVM6948 CameraCubeChip, recently commented on the significance of wired solutions in medical technology.
ECD: So now we're looking at the total systems approach.
Gunja: Many medical customers are new to CMOS, so they need some kind of data processing. Because this industry is new, we work with our partners to develop different designs. This partnership serves two purposes: It shows how it can be done. And it provides a starting point, rather than starting from scratch.
The industry is moving away from disposal medical devices towards reusable medical ones. It is a big cost-effectiveness differentiator. The way the hospital calculates it, it's a lifetime cost. To determing the cost-per-use, you calculate a lifetime cost, and then you divide it by the number of uses that you are going to get out of the device.
And if you have a reusable device, they're so expensive. A high-end endoscope can be up to $25,000. Much of this cost comes from paying a nursing and medical staff. The reason for this being, some devices could be going through maintenance or broken, thus, there is down time in actual use.
ECD: Are you addressing the cost of the electronic package pales compared to the cost of the labor crew standing around waiting for it to hit the bottom of the hole by just providing the most inexpensive solution as possible, or is this a migration towards having a more cost- effective solution?
Gunja: The cost is at par with what you would pay for a reusable device, but as single-use devices gets cheaper and cheaper, it becomes more attractive. Over time my prediction is that single use devices will get much cheaper than reusable devices. This is the reason I believe there will be a big migration. That's not to say there won't be any reusable devices left in the world, that's not to say that at all, but certain procedures will completely migrate out of reusable devices to single use devices.
ECD: How much does the recycle ability of the devices come into play?
Gunja: What happens is the handle, everything beyond it, and all the backend electronics get reused. The shaft of the endoscope, which is disconnected from the tip, is the bit that gets thrown away. This is because it's usually just plastic tubing with minimal amount of electronics. There are some products where the handle also gets thrown away. It just depends on the extent of contamination. If the handle gets badly contaminated during the procedure, and you can not guarantee that it would be cleaned properly, then there are product concepts that actually incur the cost of throwing away the entire handle.
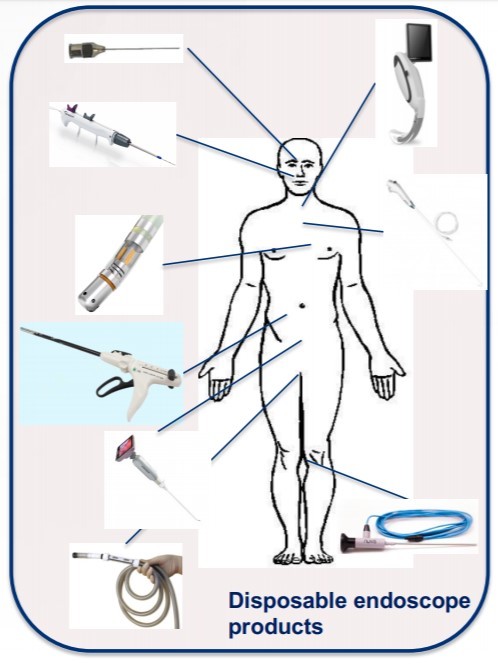
But the goal to throw away the minimal amount of electronics which can be reused. When you have an imager that small, what can you do? The first thing you can do is you can add a camera to more places so you don't have a blind procedure. You can add a camera to needles, endoscopic tools, catheter guide wires, stents, clipper pliers, to wound staplers -- literally everything including the body where you need to.
ECD: By default should any invasive tool have an optical sensor at the end?
Gunja: So that's the reason if it was in the body, it's got a camera. The camera is so small and so cheap, that the question of not putting in the camera does not arise. That the end game that we are aiming towards. Then we have something so small, because the surgeon can see, can actually do procedures which were not possible to do before. Like in the brain; in the eye; in the spine, and heart. So, you know, it opens many new doors to procedures. Makes things safer, more productive, and more targeted.
The procedure defines the diameter of the endoscope, and that defines the maximum dimension of the image sensor. Not only is ours very small, it can capture 200x200 pixels at 20 frames per second. It’s the first medical imager to use backside illumination pixel technology. Power is important, not so much because you're trying to save current or to preserve battery life, but you want to generate minimal amount of heat at the tip of the endoscope, otherwise you start burning the patient from within that way.
ECD: Are thermal issues critical at those power levels?
Gunja: You have to remember that usually there are two LEDs at the tip too, and they also produce heat. It's a system with a heat budget. You can not exceed 43 degrees celsius at the tip of the endoscope. Our customers go to great lengths to get the heat away from the tip. To get the size down in our camera module, what we did to make it more suitable for single-use applications is the lens. What we did was create a wafer level lens, which is much cheaper, for a single use device, which has comparable image quality to an all-glass lens, but is much, much cheaper. Traditionally in a reusable endoscope, the lens is made out of glass. The cost of glass lenses can be about $250 to $300. If the lens is going to be so expensive, then it precludes that device from being a single use device. So that if earlier on we recognize that the lens had a stranglehold on the growth of this industry.
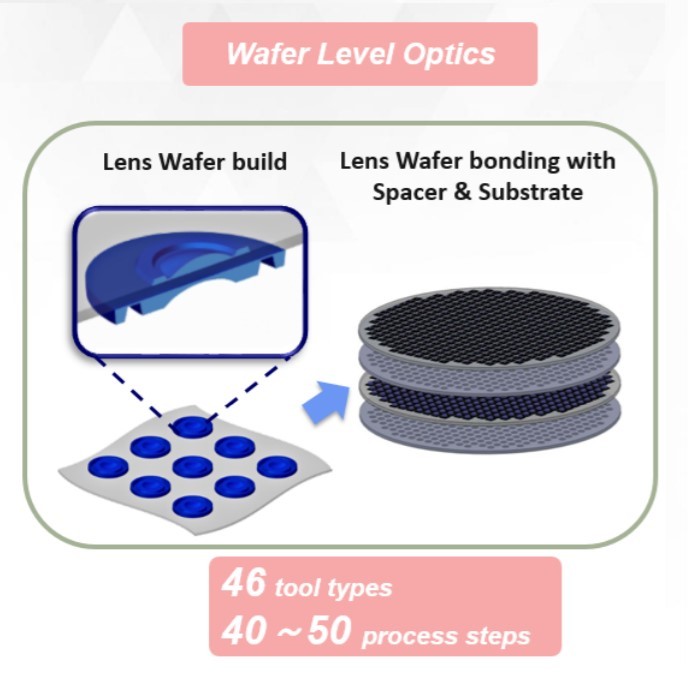
You could have 1200 to 1500 lenses on one wafer. These are plastic lenses. We then align them, fuse them together, then aligned and fused the entire lens pack onto the image sensor. Once this is complete, we cut them. You then dice them and put a black coating around them to create navigation light. The lenses are applied at the wafer level. It's quite a complex procedure that needs 46 different tools and up to 50 different processing steps, including manual steps. Once it comes out of our factory, you don't need any calibration or tuning. You can directly solder it onto a flexible or rigid PCB.
So it's .6x.6mm and can focus three millimeter to 50 millimeters, so it's quite close. You're going deep inside the body and the structures are very, very small and very close to the camera -- it has a 123-degree field of view. The colors are all accurate, you can see all of the focusing at 3mm, 15mm, and 30mm in the image. All accurate, no ionizing, no color aberration, and then even the human skin tone, which is most important.
For more information, visit www.ovt.com.